SEMINAR ON COMPUTING IN HEALTH
20 MAY 2010
DEWAN PERSIDANGAN UNIVERSITI, USM PENANG
Organiser:
USM
Co-Organiser:
MHIA (Malaysian Health Informatics Association)
Sponsors:
GE and Blue Lake Health Care
Prof Rosni Abdullah
- Re-surface of health informatics
- Launch of Telehealth under MSC
- Health Computing - elements of processing, have algorithms to analyse those data
Prof Dato' Dr Jai Mohan (jai_mohan@imu.edu.my)
Vice-President MHIA
- Overview of what has happened to MHIA
- MHIA meets every 2 months and when there is a speaker in the region
- MHIA started when 7 MSC projects were launched
- Transformation of healthcare -> Telemedicine project
- 1991-1995: admin
- 1995-1998: Information System Strategic Plan, Patient Mx Information System
- 1996-1998: Teleconsultation (urology), tele-psychitry & oncology, tele-CME
- 1999-2001: Wide area network -> Virtual Private Network (VPN), MCH Care Info System, Comm & Vector-Borne Disease Surveillance & Control System, Food Quality Control Program, first fully electronic "paperless and filmless" hospital opened in Selayang in 1999, Putrajaya in 2000 (linked to paperless primary healthcare centre)
- Downside: If don't look after it, or upgrade network, switchers, no maintenance, ....everything becomes obsolete
- Healthcare objectives -improve healthcare outcomes
- IT is for delivering over a wide area and it is achievable in the long run
- Telemedicine is slow in its rollout
- MHIA is dedicated to the development of health informatics and the utilisation of ICT to improve Malaysian heathcare services and outcomes
- IMIA (International Medical Informatics Association)
- APAMI (Asia-Pacific Association of Medical Informatics)
- MHIA: assists with the structure of educational program in medical science, promote ehealth markets
Mr Abdollah Salleh
Clinical-IT Coordinator & Consultant General Surgeon
Hospital Selayang, Ministry of Health Malaysia
"End of Cycle - What's Next?"
- The life cycle of HIS, Selayang Hospital Perspective (diagram)
- Strategic Information System Plan
- Get Funding
- Prepare Request for Proposal
- Select a Proposal from Vendor
- Work with Vendor to Customise and Implement
- Data Migration
- Operations Management
- Hardware Maintenance (Repairsm Replacement, Additions)
- Software Maintenance (Patch, Version, Upgrade, License management)
- Review System Viability
The Life Cycle of a System
- any product goes through cycle of birth-growth-maturity-death
- this is true of hardware: design, manufacturing, installation, operations, manitenance and BER (beyond economic repair)
- software should be usable forever
--content and method
--users refuse to use
--obsolete and does not fit in with new software
- Radiology Information System (RIS)-Picture Archiving and Communications System (PACS)
--software change, new product offered
--old software no longer supported
--inability to replace broken down hardware due to obsolescence: obsolete technology, no longer in production, parts cannot be sourced - eg RAID server, juke-boxes to read Optical Disc
--eg hardware: viewing station - proprietary product, no longer in production
Clinical Information System CIS-EMR
- fialure to keep up with patches, upgrades and versions
--first user of first version 1997 (15 releases since)
--now stuck in version 2002.002
- current version no longer supported
- difficulties in upgrading lead to procrstination
- failure to keep up with increasing demands for memory, storage ansd speed necessary for new versions
--no planning for system sickness and mortality
--inconsistent funding (seen as always asking more more money)
--eg HP AlphaServer systems using OpenVMS OS are being phased out
What's Next?
- Strategic Information System Planning
- Situational Anakysis and Needs Assessment
- Translate Request for Proposal
- Preparation ???
Computerised Clinical Information System - Objectives
- facilitate communication between care providers through information sharing
- enable work process automation via HIS
- gather and display vital clinical information
Challenges Faced
- Major issue: Would clinicians use the HIS?
- Achieved paper-less but not paperless
- Need speed for system performance (infrastructure)
- Underestimate huge cinical data
- There are Structured and Unstructured Data
Structured Data
- adherence to a unifrom system
- eliminate typographical errors
- ensure uniformity in use of terms
- analysis - differentiation, trending, counting, grouping of data
Components of HIS
(diagram)
Operationalization of Care Plans
- to be constructed based on pre-planned
Use of Care Sets
- order sets for each patient
Data Analysis
- Active Operations data
- Secondary dB has analytical data for epidemiologists, researchers, etc
- Analysis of aggregated data
Health Management Information System
System Generated Data
Automated Transfer of data to external dB
Data Retention and Data Migration
- retaining data for the enterprise
- moving data between 2 systems
Upgrading Project Timeline
- will continue to use the Patient Mx System, Clinical Info System, LIS for at least 2 years
- things will improve because of new clients, printers and network
- new RIS-PAC and the ubiquitous Web Client
Implementation Dilemma
- RFP is equivalent to stating the SISP
Change strategy
- what to do with the old
- keep in functioning order for as long as we can
- use a parallel system during implementation
- use for data retention when data migartion is not possible
- if whole system cannot be salvaged, use whatever can
Dr Cheah Yu-N
- HIRG was formed in 1996
- Areas: intelligent systems, knowledge discovery, neural networks
- MSC Telemedicine pilot projects
- Research areas: Telemedicine, Knowledge Mx, Health & Wellness, Bioinformatics, Image Processing
Telemedicine
- Tele-healthcare information & diagnostic environment (TIDE)
- web-based advice system
Knowledge Mx
- Dynamic personalised planning - eg for renal disease
- Can be extended to personalised lifetime health plans (PLHP)
- Enriching medical PBL with tacit knowledge
--PBL problem composer and presenter
- Strategic knoweldge services
--To derive knoweldge from data and to use it for strategic decision-making
--Data mining
- Converting structured and non-structured documents into reasoning structures
--eg EMR into cases (for case-based reasoning/evidence-based medicine)
- Coalition formation
--Forming cohesive teams for specific healthcare tasks (eg surgery)
--Based on profile, personality, etc
People and Organisational Issues
- IT Adoption in EMR
--Whether workers will use EMR
- E-Health System
--eg Cancer Community Portal
--eg Diet Portal
- Privacy in Health Informatics
--Explore privacy issues among patients and caregivers
Medical Imaging and Visualisation
- Automatic 3D landmark detection and placement
- Crest Line Extraction (Heuristic method)
- Crest Line Registration
Health and Wellness
- Personalised healthcare information (PHI) delivery
- Virtual Health Connect (Jasy Liew Suet Yan, Ooi Keng Siang, Matthew Phiong, Loo Wan Koe)
- "Team Cosmic Malaysia" - demo
--1st place (Unlimited Potential Design for Development Award)
--Microsoft Imagine Cup
--Worldwide Finals 2009, Egypt
-- TEA BREAK --
Puan Maria Sidi
UMMC
Managing ICT Health UMMC Experience
Managing ICT -
5 keys areas--IT Governance
--System and Infrastructure Lifecycle Mx
--IT Services, Delivery & Support
--Protection of Inf Asset
--Business Continuity
- Why are these 5 areas important? They are interdependent and you must have them all in place
Objective in Managing ICT
- Information Criteria
--Effectiveness
--Efficiency
--Confidentiaility
--Integrity
--Availability
Managing IT Resources
- Must meet enterprise goals
- Governance Drivers
- Business Outcomes
--Applications
--Information
--Infrastructure
--People
- IT Processes
- IT Goals
Managed Infrastructure
- KPI for information retrieval is 3 secs
- So if an ifo structure can't give info back within 3 sec, users will refuse
- An enterprise must manage own IT people, their KAP & Skills
Maturity Level in ICT'
Scale & Description (table)
0-Non existent
1-Initial/adhoc
2-Repeatable but intuitive
3-Defined Process
4-Mananaged and measurable
5-Optimised
Critical Success Factor in Managing ICT
- User Commitment
- Good Project Mx
- Return on Investment (ROI)
- Bottom Up Mx
ICT in Healthcare
- Improvement of process and regulatory
- Integrate all processes of patient mx
- Patient safety, esp verification of info
--ie the system must VERIFY that this is the CORRECT patient
--eg patient named 'Maria' but 'binti' can be different for different patients
--eg even if names & surnames are the same, the birthdates & addresses are different for different patients
--eg the same patient goes to several clinics and this must be picked up by the HIS
- Standards of coding for statistics
- Analysis of patient and tx info
Health Informatics Objective
- ICI Standards - Information Resources Mx Comm
- Data needs Across the Health Continuum
- Quality Information for Decision Making
About UMMC
- Statutory body under the MoHE
- Provides public services, edu & res for PG & lecturers
- Satff Information
--Current # of staff: 4,300
--Student: 1,000
--Beds: 900
Patient Stats
Jan-Dis 2009:
in-patient: 62K
Out pt: 706K
Ave daily pt stat (2008)
in-pt: 173
Outpt: 3,200
UMMC Business Vision
- Paperless organisation
- Seamless flow of information
- Reduce resources, inc quality of services
- Data mining for res
- Accreditation (ISO, JCI, MSQH)
Hardware and Infra ICT
PC 1675 units
IT Governance - UMMC ICT Policy
- Dasar Keselamatan Perkakasan IT
- Dasar Keselamatan Perisian dan Aplikasi
- Dasar Keselamatan Rangkaian dan Wireless
- Dasar Keselamatan Data & Maklumat
- Dasar Pengunaan E-mel
- Dasar Pencegahan Serangan Virus
- Dasar Pengunaan Internet
Implementation of 5 Key Areas
(table)
- Clinical Applications
--MPI
--ADT
--Appointment
--Billing
- Clinical Support APPLICATION
--PIS
--LIS
--CCIS
--PACS/RIS
--Maternity
- Non Clinical Applications
--Portal pelajar
--Portal PPUM
--Finance & Inventory
--eHR
--GOE
--EMMS
--Single sign-on
Protection of Information Asset
- dB Audit
-- tracks whoever logins, editing, deleting, amending
- Single sign-on (SSO using staff #)
--GOE (letters, cuti online, etc)
- Proxy System
--for tracking users, so that system is not congested
Data Recovery
- Storage and Critical Server Availability
- Archiving (Replication Archive Storage and DICOM Image Availability)
- Virtualization Machine (VM)
Where is UMMC?
Governance (to meet JCI & MSQH stds) 3
System and infrastructure Lifecycle 3
Service Delivery 5
Security 3
Business Continuity 3
Challenges - Issues & Action
- Process owner do not know what they want - Mx user expectation
- Rqmts - ??
Lessons Learnt
Moving Forward in ICT
ROI
- Cost of films
- Cost of papers
- Ratio of resources (staff: support)
- Waiting time (esp for film & report)
- Competency of ICT
Assoc Prof Dr Noraini Abdul Rashid
Parallel Algorithm Computing Group, School of Computer Sciences, USM
Bioinformatics
- DB is a collection of info in a structured way
- Bioinformatics deals with many forms of data
- EMBL-EBI
http://nar.oxfordjournals.org/content/vol30/issue1/
- FIG3: James Ostell, Databases of Discovery, Queue Vol 3, Issue 3 (April 2005)
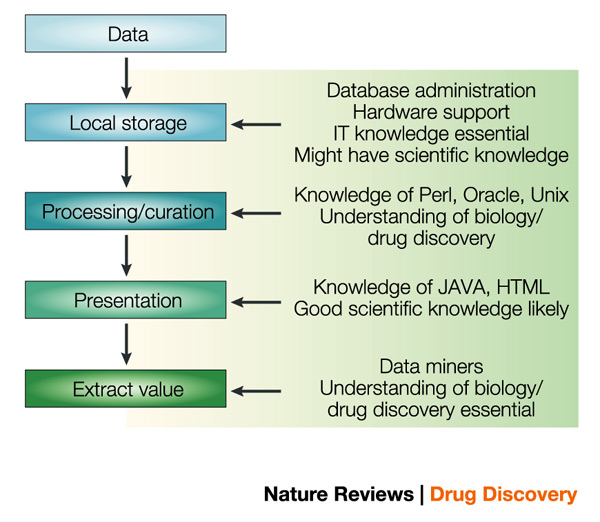
- Nature Review - Drug Recovery
http://biointelligence.files.wordpress.com/2009/08/nrd1356-i11.jpg
What is Bioinformatics?
Computer science
Genomics
Statistics
Computational Biology
http://sciblogs.co.nz/code-for-life/files/2009/12Bioinfo-flow0chart.jpg
Bioinformatics Framework
- Doping Centre, USM workflow
Focus Areas
- Sequence analysis
- Biological Data Mx
- Image Processing
- Biological Data Analysis
Medical Data
- Medical
- Dx
- Hospitalizations
- Referrals
- Contacts
- Analysis (records)
Research Projects
INFONatRes Engine: A portal of integrated molecular dB
- Framework (diagram)
- Novelty - new application
- Can search 2D and 3D, eg photo of a plant -> its active compund
Implementation of Mediator-based Integration System for a Transparent Access to Multiple Biological dB
- Wahidah Husain, Nur'ani Rashid
- unified access to biological info
- user only needs to interact through a single schema
- mediator-based system: can unify different data formats
SEQAlign - Implementation...
- this is a plug-in tool
Visual data Preprocessing for medical dB
- heart patient's data from IJN, KL
- Demo & op details
Diabetes Detection System
- Mohd Adib Haji Omar
- to analyze patient's data (a prediction system)
- doctor can select patient's data
- dx based on the patient's data
-- LUNCH --
Ms Pat
Clinical Radiologist
TeraRecon, Inc
Simple solutions for complex data
Workflow-based 3D Applications
- eg head to foot body scan @0.8mm = 1,792 slices = 1 volume of data
- digitised x-ray looks like the real x-ray but can magnify, reduce, contrast brightness, do measurements, etc
- with new technology, can organise by modality
Vessel manipulations
- eg data of a vessel from a cardiac path lab - can manipulate the data we see
- eg doppler ultrasound (a different modality) of the same blood vessel of the same patient
- eg the pc converts the images from 2D to 3D, and we can manipulate the data, do editing, crop away areas we don't need, etc
- use automatic algorithm to analyse the 3D image
- if suspect a stenosis, use a curve algo to follow the vessel and alert us to a problem with the vessel
Skull manipulations
- bone not picked up could be calcified mass
- cavernous sinuses - no plaque on vessels
Orthopedic manipulations
- If given access, can do a lot of things
- Can host the image for tele-consultation
- Can have multiple users, all seeing the same image
- eg shattered hip in a patient
Aquarius (software)
- eg want to remove bones from an image and just leave soft tissue
- eg origin of coronary artery
- Can change the workflow and use the workflow of others
- Cannot apply to abnormal anatomy (will only work for normal anatomy)
- eg images from Grey's Anatomy
- What is LAD?
- Software should be able to tell user which was done by the PC and which was done by humans
- Cannot always trust a software; must always check that it is doing things right; always check back with source data
Functional Analysis
- Software should be able to tell us what we are dealing with
- It should be able to identify what object we are dealing with
- "zero download", there is no footprint, but there is a url
- Our fellow clinicians can see the same image but others can't
Networked Products
- Products are all web-based and users can access them online
3D Re-Construction
- eg metallic artefact can be verified in other images
- eg blood vessel or BBQ fork at below knee can be an artefact
- eg ribs were not broken despite severe traumatic injury sustained by a patient
Q&A
1) What API is being used? Rendering at this high resolution and at this fast speed, what did you use? Is there a graphics library being used? Use eCard to do rapid hi-res rendering.
2) Re colonoscopy. First generation colonoscopy software. Has negative predictive value (ie useless for predicting colon cancer). Patients can be subjected to virtual colonoscopy.
3) Politics vs Human Nature.
4) What is unpleasant colonoscopy? Inflate the colon for colonoscopy with CO2 -> experience cramps -> while being investigated. CO2 then has to come out the same way it came in.
5) Intelligent CT Scanner that can do bone removal from the images and label each bone or digit. However, it cannot tell abnormal structure and artefacts; it only knows normal.
Dr Nasriah Zakaria
School of Computer Sciences, USM
Certification Program in Biomedical Informatics
- Senior Lecturer
- Biomedical Engineering (1997)
- PhD Information S&T (2006 USA) - Health Information Privacy & Disclosure
- Social Computing Lab, Comp Sci, USM
People & Organisational in Health Informatics
--IT Adoption in EMR
--Privacy Issues in eHealth
--Sociability Issues in eHealth System
--User Acceptance in Telemedicine
Terminology
- Biomedical Informatics
- Health Informatics
- Medical Informatics
- Core is "Health IT"
- Stakeholders are clinicians, nurses, administrators, computer scientists
US Scenario
- Interest based on US leadership - President Bush
World Scenario
- UK spent 11 billion pounds nationwide for EMR for all citizens
- Australia - Healthconnetc program
- Sweden, Germany, Norway, France
- Asia - Japan, India, Malaysia, Singapore
AMIA 10x10
- AMIA (American Medical Informatics Association)
- "10 x 10" means reaching a target of 10K people by 2010
-
https://www.amia.org/10x10
-
AMIA 10x10 Goals
- To cretae sufficient workfornce to support Biomedical Informatics
- To expose participants to a s et of Biomedical Informatics concepts
- To learn how to .....
Participating in 10x10
- Register with AMIA and pay for course
- Listen to lecture online, read textbook, do weekly quiz, prepare Course Project
- Present Course Project, get certificate
AMIA Training
- Can go through Unit Latihan, USM
- Fees (RM6,389 or US$2,000) and travel to USA (Jul-Oct 2010)
- Write report
- Course are listed at AMIA website
- Instructor: Professor William Hersh
- Textbook: Shortliffe EH, Cimino JJ "
Biomedical Informatics: Computer Applications in Health Care & Biomedicine (2006) 3rd edition, Springer.
- Topics
--Overview of Field and Problems Motivating It
--Biomedical Computing
--Electronic and Personal Health Records
--Meaningful Use of the EHR
--Standards and Interoperability; Privacy, Confidentiality & Security
--EHR Implementation and Evaluation
--Evidence-Based...
Week 7: Information Retrieval & Digital Libraries
Sample Discussion for Credit:
Choose a question related to biomedicine ...
Course Project
Do an organisational scan
Face to face
San Diego, USA, 19 January 2010
Project Overview
- Bkgr
- Case Study
i10x10
- International 10x10 version
i10x10 in Singapore
- 20-30 Singaporeans have done this course
- this course is endorsed by the Singapore Govt
Certification
- still under discussion
- Certification will help to build the bioinformatics workforce
- MSc, PhD Health Informatics (graduate under Computer Science)
Assoc Prof Dr Mandava (mandava@cs.usm.my)
School of Computer Science, USM
Medical Image Visualisation
- ENDEAVOR (
Exte
nsible Me
dical Imag
e Analysis)
- ENDEAVOR is a plug-in tool
- It can be used by anyone who uses medical images
- Demo: White matter lesion (how ENDEAVOR can be used for free text annotation which can be transmitted and can be shared by multiusers, etc)
- Currently working on bone tumors (osteosarcomas)
- Intelligent retrieval of medical images form PACS
Dato' Teddric John Mohr
DSPN
- Joint Commission International
- 6 hospitals in Malaysia have accreditation
PAH Today
Penang Adventist Hospital
- Revenue RM28-165 million
- Outpatients 900 per day
- Most doctors are from Singapore
What does the patient want?
- Outcomes (patient defines this)
- Highest quality (the right doctor, equipment staff)
- Lowest price
Corporate Model = BOARD
- Delegate Quality of Patient Care
- Bylaws
- Patient Care Review Committee
PAH's Quality Initiatives
- AMI - reduced by 37.6% from mean of 10.1% to 6.3%
- 57 studies on-going (@10 a month, every nurse and doctor is studied)
- IHI Golden Trigger Rules
- 10 beds in ICU/CCU
PAH IT Framework
- If you have data, you can have quality.
- You cannot have quality without data!
- You must collect data and analyse that for your records!
- Everything is now done digitally to minimise errors
- Breast cancer requires the best resolution to detect even a small abnormal spot that could be indicating a malignancy
- In the old days, EKG was jaggered. But today it is smooth.
- 50% of blindness is diabetic. Diabetes is an expensive disease!
- It is how long your patients live that matter (they don't go on TV to tell the truth)
HIS
- HIS must be able to track everything 24/7 and report to you 24/7
- You cannot afford to lose data if you have a HIS
- You cannot report that you have data 24/6
- Loss of patient data is fined US$10,000 per patient
3-Tier Hardware Architecture
- What is a 14/92 IBM? That is for relay. This is a cluster...
LIS
- Dedicated Lab System to generate accurate lab result
- Linked with HIS system
- Linked with Lab Analysers
Medication and Supply Automation
- Medication Automation System (pharmacy)
- Supply Automation System (supplies)
- this gives better inventory and billing control
- Malaysia requires stringent control on such aspects
- You know exactly what comes in and what goes out
RIS/PACS (Oct 2005)
- RIS (Radiology Information System)
- PACS (Picture Archiving Communication System)
Benefits of PACS
- Faster throughput
- Less waiting time for patients
- Can transfer images to UK and other countries fast enough for interpretation
- CD Burner (sometimes patients want their images, this is illegal to give away)
- Film Digitiser (looks like a big printer)
- Once digitised, you can store the digitised films for long enough
EMR (Electronic Medical Record)
- Emergency Dept
- Outpatient
- Inpatient
- eg Denver, Colorado
- eg ALERT by Cerner, is a world-class system. It is a touch-screen system and doctors like this very much. All they like to do is touch, touch, touch!
Challenges
- Change Mx
- Quality & Cost
-- eg Oncology
-- People cost 60%
-- IT cost 2% of the lifetime of a hospital
- USA Medicare - no payment for re-admission
-- eg Oncology need treatment and post-treatment
- Superefficiency
--Technology is the future
--You cannot go into the future without technology
Q&A
1) Who owns what? Answer: In Malaysia today, the doctors own the information of his/her patients. The patients can get their medical info but they cannot get the films or charts. The hospital owns the films and charts.
2) How did the private hospitals use HIS? Answer: No HIS, no $$$. Some doctors are ready, some are not. Doctors are very competitive and they don't want to be left out. They will want to own what other doctors own.
3) Who can watch patient treatment? Answer: It is cheaper and saves $$$ if you do it together using IT (saves RM30million?)
4) Health outcomes. Answer: Joint Commission Survey - must not talk about the patient or any of the hospitals. It must be kept secret. Virtual colonoscopy (goes in the other way and up), Pill Scan (goes in at the intestine), etc
5) Patients' Privacy. Answer: You have to guard that as some patients are high profile, including PM's wife.
Ms Susan Barnes (NZ)
GE eHealth Solutions
eHealth & Healthcare Transformation
4 Common diseases
- increasing healthcare cost (aging population, chronic diseases)
- inefficiencies (scheduling, payment)
- lack of access (too few doctors in rural areas)
- unsatisfactory quality (incomplete data, medical errors, etc)
Australia
Federal budget AUD$467 million
Defining the Connected Healthcare Ecosystem
- ehealth ecosystem
- health information exchange infrastructure
- health record banks
-








{kind=link}
{kind=link}